The Differences among Characteristics of Mesenchymal Stem Cells from Different Sources
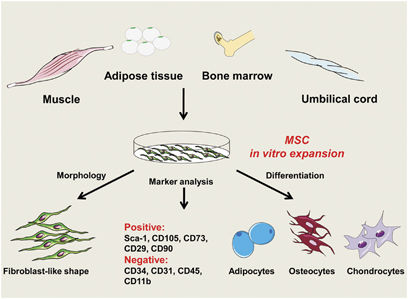
Mesenchymal stem cells, also called MSCs, are multipotent stromal cells that can differentiate into a variety of cell types, including osteoblasts (bone cells), chondrocytes (cartilage cells), myocytes (muscle cells) and adipocytes (fat cells which give rise to marrow adipose tissue). MSC have been found in organisms (in-vivo) and have been studied as well in tissue culture (in-vitro). Mesenchymal stem cells (MSCs) were first found in the bone marrow and widely distributed in the human body. Although mesenchymal stem cells from different tissues can meet the minimum standards (definitions) set by ISCT, there are still many studies that suggest some differences in MSCs derived from different tissues, mainly reflecting in the proliferation rate, secreted cytokine profile and immunomodulatory capacity. The repair function for damaged tissues of Mesenchymal stem cells work through sequestering cytokines, reducing inflammation, reducing apoptosis in tissue cells, eliminating fibrosis in order to promote the proliferation of stem and progenitor cells of endogenous tissues and organs, so as to achieve the effect of repairing tissues and organs, instead of through cells that differentiate into tissues and organs (autologous mesenchymal stem cells may be involved in differentiation mechanisms). Therefore, we will focus on the differences of MSCs that derived from separate tissues in the content, proliferation, immunomodulatory capacity, and secretion of cytokine profiles. Differences in MSC content from different tissues According to the CFU-F experiments, bone marrow MSC content of mononuclear cells accounts for about 0.001% to 0.01%, whereas placental amnion and umbilical cord MSC account for about 0.2% to 1.8% of mononuclear cells. In addition, studies have shown that MSC content is as high as 80% -100% in mononuclear cells isolated from amnion and umbilical cord; however, only 8% of mononuclear cells isolated from cord blood are MSCs. The very small number of MSCs in umbilical cord blood resulted in a probability of 5.7% to 10% for successful isolation from umbilical cord blood. It is unclear what fraction of MSCs are in the single-cell fat digest, but relevant studies suggest that it does not exceed 50% and that this 50 % contain endothelial cells, adipose stromal cells. MSC in different parts of the umbilical cord (umbilical cord, umbilical cord, umbilical cord peritumoral, and Huatong gum) were different to some extent even with umbilical cord sources. Wharton's Jelly has the highest MSC content and the strongest proliferative capacity. Differences in proliferative capacity of MSCs from different tissues Bone marrow-derived MSCs are the most widely studied and therefore bone marrow MSCs are often the target of comparative study for mesenchymal stem cells derived from other tissues. It takes 15-22 days for P1 generation cells after the separation of adipose MSCs and bone marrow MSCs, but it takes 30 days for cord blood MSCs to grow. After P1 generation, doubling time of amniotic fluid MSC (the time needed to double the number of cells) was 1.6 days while the doubling time of bone marrow MSCs was 3.75 days; the proliferation ability of adipose MSCs was close to that of amniotic fluid MSC, still better than the doubling time (About 44 hours Vs about 76 hours). . There are also studies showing that proliferation of human umbilical cord pericytes MSC did not differ significantly from that of human bone marrow MSCs before passage 3 of the culture; however, the doubling time of umbilical cord perivascular MSCs was significantly shorter from the 7-14th day (after passage 3) In bone marrow MSC. The doubling time of umbilical cord MSCs was shorter than that of placental MSCs, indicating that umbilical cord MSCs are superior to placental MSCs in proliferative capacity. The same algebraic bone marrow-derived mesenchymal stem cell that had the weakest colony-forming ability compared to the umbilical cord, umbilical cord blood, and amniotic membrane. Clonal growth capacity can be used as a more important indicator to evaluate the quality of mesenchymal stem cells. Under the same laboratory culture conditions, bone marrow-derived MSCs can only be expanded to passage 10, and the umbilical cord, umbilical cord blood, and amnion-derived MSCs can only be expanded to 12-14 passages. Even laboratories can do umbilical MSC cultured effectively expanded to 40 generations, still has a multi-directional differentiation potential. Cell karyotype analysis showed that chromosomal abnormalities and telomerase shortening occurred in MSCs cultured to passage 18, while umbilical cord MSCs developed chromosome abnormalities until 30 passages. Regardless of the tissue from which MSC originated, they did not find tumor cells characteristic of gene mutations after amplification of multiple generations in vitro. MSC involves age characteristics, the number of bone marrow MSC and proliferation decreased significantly with age. Interestingly, gender also affects the size and proliferation of MSCs. Differences in the immune regulation function of MSC from different tissues Umbilical membrane-derived MSCs have lower immunogenicity and stronger immunomodulatory effects than those of bone marrow MSCs, and the inflammatory environment can improve the expression of HLA-DR of bone marrow-derived mesenchymal stem cells. MSCs (P2 generation) and CD3 + T cells in 1: 1 co-culture experiments showed that MSCs and umbilical cord blood MSCs significantly inhibited the proliferation of CD3 + T cells compared with the control group (no MSC group), while placental MSC only slightly inhibited CD3 + T cell proliferation. Differences in MSC secretion factor profiles in different tissues Umbilical cord blood MSCs secrete more cytokines that support hematopoiesis, thus supporting hematopoietic stem cell clone formation better than bone marrow-derived mesenchymal stem cells. However, studies have also shown that the ability of bone marrow MSCs to promote hematopoietic stem cell clone formation is superior to cord blood and umbilical cord sources. The cytokines (G-CSF, GM-CSF, HGF, IL-6, IL-8 and IL-11) secreted by umbilical cord MSC are much higher than that of bone marrow MSCs, but the amount of VEGF secreted by bone marrow MSCs is higher than that of umbilical cord MSC. The phenomenon of high expression of HGF and low expression of VEGF by umbilical cord MSC was further verified in another independent laboratory. This shows that bone marrow MSCs have some advantages over umbilical cord MSCs in promoting angiogenesis. At the genetic level, fat-derived MSCs express BDNF in a higher amount than bone marrow MSCs, but bone marrow MSCs express higher levels of NGF. Commercialized bone marrow MSCs and adipose MSCs had similar proliferative and chemotactic abilities, but there was a significant difference in proliferation and chemotaxis between adipose MSCs from different individuals cultured in the laboratory. Conclusion A.MSC content in the tissue (cell abundance): the umbilical cord content is undoubtedly the highest, followed by amniotic and fat; while the umbilical cord blood content is very small, resulting in undetectable occurrences B.MSC Proliferative Capacity: Due to the age-specific characteristic of MSCs, umbilical cord and amniotic-derived MSCs have distinct advantages in that fat and bone marrow are secondary. C.Immunomodulatory capacity: MSCs derived from umbilical cord, amnion and adipose tissue were superior to those from bone marrow MSC, whereas placental MSCs possessed the least immunomodulatory capacity. D.Secretion cytokine profiles: The total amount of cytokine secreted by the umbilical cord MSC was significantly higher than that of the bone marrow MSCs, but the secretory cytokine profiles from different sources had distinct characteristics Due to the advantages of easy access to source and high proliferative capacity, mesenchymal stem cells can be cultured to obtain a large number of MSC cells that is sufficient to meet the clinical treatment needs, making the most suitable umbilical cord, amniotic membrane and fat as the source of tissue for MSC therapy. However, we must recognize that different laboratories, different isolation methods and different culture systems may lead to inconsistencies in the experimental results of MSC. Even if the same source, There are functional heterogeneities in mesenchymal stem cells between different individuals. That’s why scientists must be cautious about the current findings and conclusions. We believe that a breakthrough in technology development in the near future can offset the differences in MSC functions caused by differences in tissue sources. Related products: Mesenchymal stem cells
Your email address will not be published. Required fields are marked *